


A deep ache.
A throbbing, pulsing pain.
A worrying wrongness high in the back of your thigh, right where it meets the base of your buttock.
If you’ve felt this before, you know the mental spiral that comes with it. The restless nights trying to get comfortable. The concern when it shows up after a walk, a ski day, a bike ride. The quiet fear that something fundamental has changed.
In today’s post, I want to do two things clearly and honestly:
Help you diagnose the true source of activity-related buttock pain, and
Show you how to restore that tissue to something quietly capable and trustworthy again, without guesswork or unnecessary rest.
You’ll learn how to avoid babying this injury and how to understand it well enough to load it correctly.

Why these injuries show up more often as we age
I spend a lot of time solving soft tissue problems and understand the unique challenges we face as aging athletes. Muscle and tendon strains aren’t exclusive to athletes over forty, but they do become more common and more confusing as we accumulate years of training, living, and adapting.
That’s not a character flaw. It’s physiology.
I want to delve into this briefly because we’ll use the same strategies shared below for other injuries we’ll cover further into the publication and I want you to understand. Soft tissue changes are one of the core challenges we face as aging athletes.
So what happens?
When researchers compare injury patterns across age groups, a consistent trend emerges:
Younger athletes tend to experience high-energy injuries: ligament ruptures, joint trauma, clear “snap” events. If there’s an overuse event it’s typically clear and obvious, and heals quickly with little additional help needed.
Older athletes trend toward soft-tissue and tendon injuries: gradual onset pain, overuse patterns, spontaneous strains that seem to appear without a single inciting moment. Classically “i just woke up with it”, or “same activity, different day, and now it hurts” are common complaints.
The reason lives in our connective tissue and the predictable and modifiable changes it experiences as we age.
Younger tissues contain a high proportion of well-organized type I collagen with strong cross-links between fibers. These tissues are strong, stiff, and resilient—until they fail, often suddenly. I think of old-school denim versus the stretch jeans we wear now: the kind you had to lie on the floor to get into and peel off at the end of the day. They didn’t give much, but they were nearly indestructible.
In the same way, younger muscles are powerful, connective tissues are robust, and the system as a whole tolerates abuse remarkably well. Like those beloved jeans that lasted for decades, it holds up—right until it doesn’t.
As we age, several things begin to shift.
Collagen production becomes less efficient. Fibroblasts still produce collagen, but it is more disorganized, thinner, and mechanically weaker. These are not abstract changes. They have real consequences. The same structures are present, but it now takes less force to cause damage.
Elastin content declines, reducing the spring-like recoil that once protected tissues during rapid loading. With less elastin, there is less “give” in the system and fewer small shocks absorbed along the way. Think of the suspension on a mountain bike: when it’s working, you barely notice the terrain; when it’s not, every bump travels straight into the frame.
Advanced Glycation End Products (AGEs) also accumulate, creating non-enzymatic cross-links that make tissue feel stiff without actually making it strong.
This creates what I call the “stiff but weak paradox.”
You feel tight. Motion feels restricted. But the tissue’s ability to tolerate load has actually decreased.
Add to that:
Reduced tendon cell turnover - we don’t make new tendon cells to replace damaged or weakened ones as quickly or productively
Slower repair of micro-damage - the small traumas inflicted by just living and being take longer to heal
A growing mismatch between muscle force and tendon tolerance - muscles can retain or re-develop great force production qualities, often much faster than tendon tolerance can increase leading to quietly vulnerable connective tissue if we haven’t done the prep work
Changes in blood supply in so-called “watershed” areas such as the shoulder and achilles
And suddenly, a perfectly normal training load or activity can exceed a tissue’s current capacity.
Are these changes reversible?
Partially—and in meaningful, felt ways. That’s the good news.
You can’t rewind tissue age entirely. But you can change tissue behavior, structure, and resilience at any age if you apply the right signals in the right proportions.
When a close friend recently strained her hamstring high near the buttock, her questions were exactly the ones I hear in the clinic every week. I’ll answer them below and we’ll use this opportunity to look closely at this specific injury and at the broader principles underneath it—principles that apply not just here, but to nearly any soft-tissue injury that shows up as we keep training and living. This way you’ll have a rough template you can begin to apply to your own twinges aches and pains.
When this kind of pain appears, the questions I hear are usually very practical:
Should I be stretching this?
How long does recovery usually take if there was no obvious tear?
Should I stop biking or skiing if I feel it during activity?
Is massage helpful—or could it make things worse?
Before answering any of those, let’s take a look at the specific tendon involved and how we diagnose it. Everything that follows depends on treating the right structure.
Diagnosis: Glute or High Hamstring?
This injury can be confusing. The pain sits in just the right place for a glute tendon insertion injury, and it often hurts simply to sit on—something we don’t usually associate with the hamstring.
When most people think “hamstring,” they picture an athlete sprinting across a field or down a track, suddenly pulling up in agony, hand clamped to the back of the thigh. They don’t picture someone rubbing their sit bone like they’ve sat on a thumbtack, or subtly shifting their weight during a long car ride or flight, trying to escape a deep, nagging ache.
And yet, that presentation fits a high hamstring strain remarkably well. As you’ll see, there are several clear factors that help us dial in the diagnosis and make sense of why this injury feels so different from what we expect.
So why NOT the glute? The gluteus maximus is the largest muscle in the human body. It’s short, powerful, and designed for explosive force over a relatively small range of motion. True overuse strains of glute max are very rare. It’s just too powerful and we don’t typically do heavy things accidentally in the ranges where it’s weakest (hip full flexed or full extended).
The other smaller gluteal muscles — glute medius and minimus — do strain, but when they do, pain tends to show up along the side of the hip, often toward the front of the pelvis, not deep at the base of the buttock where you sit.
High hamstring tendons, on the other hand, are a perfect storm:
Long, slender tendons
Crossing two joints
Loaded heavily during acceleration, deceleration, and forward lean
Vulnerable to age-related collagen changes
Deep buttock pain that worsens with running, skiing, sudden accelerations, or changes in direction?
Gradual onset soreness without a single “pop”?
Pain that’s aggravated by sitting, hinging, or long strides?
That profile fits proximal hamstring strain far better than a glute injury.
Once the diagnosis is clear, the path forward simplifies.
Treatment: What actually restores hamstring resilience
To come up with the best and truly transformative rehab plan we can lean on decades of work from sports where hamstring injuries are common and costly. Soccer alone has driven enormous investment into understanding what actually reduces recurrence and accelerates healing, and those principles will apply just as well to us when we adjust the load and the recovery timeframe expectations.
From that body of work, several core principles emerge consistently.
1. Start loading early — gently, but deliberately
It is safe — and beneficial — to begin isometric loading within 2 days of a strain.
This may be a surprise to many. Studies comparing early loading (within a few days) to delayed loading consistently show faster overall recovery and better tissue organization when loading starts sooner. And this is not a small effect, the time to return to sports is significantly faster when we start sooner.
I’ve been in practice long enough to remember learning the classic three stages of recovery. If you’ve taken any physiology, you may remember them too: acute (3–5 days), sub-acute (5–21 days), and chronic (21+ days).
For a long time, this was the roadmap. We predicted healing based on calendar days from injury and made decisions accordingly. It made a certain kind of sense to wait until the acute and even the sub-acute phase had passed before introducing meaningful load.
If that’s been your mental model after a strain, it’s time to update the software.
We now know we can and should begin loading much sooner. And when done correctly, it’s not just safe. It’s beneficial.
Video Credit: https://www.precisionphysio.com.au/youve-injured-your-hamstring-what-now/
Begin with simple isometrics:
Lie on your back
Heel on an ottoman or chair
Press down gently and hold 20–30 seconds
Repeat 4 times
Perform 1–2x/day
Gradually work into longer muscle lengths by increasing knee extension.
Pain should not spike after these contractions. Mild discomfort that settles within 20 minutes is acceptable and expected.
DO NOT SKIP THIS EXERCISE! Doing isometrics can sometimes feel like watching paint dry, but stay diligent and do them. In the early stages they are simply the safest way to introduce and increase load on your body and to scale the load up to the point where it matters and where you can begin to add more dynamic movements.
2. Progress toward hip-dominant strength
As tolerance improves, transition to hip-centered loading. Since the hamstring crosses two joints, the hip and the knee, it functions to control both joints. Hip-centered loading simply means doing motions that are generated or directed by the hip rather than the knee. This group of exercises will include:
Hip thrusts
Bridges
Romanian deadlifts
Split squats or lunges (as tolerated)
The goal here is not fatigue. It’s restoring force transmission through the hamstring–glute complex.
Since this is a high-hamstring injury we’re fixing, these hip-dominant moves are even more important.
3. Add knee-dominant hamstring work
Since most activities also involve the use of both the knee and hip, it’s important to include at least some knee-dominant strategies to strengthen the entire kinetic ‘chain’. Ignoring one end of the muscle leaves you vulnerable.
Effective options include:
Supine ball bridge curls
Slider curls
Assisted Nordic hamstring lowers (if appropriate)*
*Nordics are powerful but demanding. They’re not mandatory early, and they’re not a badge of honor if the strain is simply too high.

4. Reintroduce general conditioning intelligently
If tolerated:
Light jogging
Uphill hiking
Low-intensity cycling
Avoid aggressive accelerations and direction changes until strength work and jogging feel stable, even if mild soreness persists.
Use a symptom-based progression:
Mild soreness during activity is acceptable
Symptoms should not worsen and should settle within ~2 hours
The high-impact levers that matter most
This is where errors of omission and proportion matter most.
For active rehab-minded adults with good self-care habits, much of what I do in the early stages of the diagnosis is to fix these errors.
An error of omission means you’ve simply neglected to include an important step or rehab mix ingredient, like isometrics.
An error of proportion means you’ve been doing the right things but with the wrong priorities or focus, for example spending lots of time and energy on massage and passive modalities and breezing through the exercises without making sure you are consistent or are ramping up the intensity progressively.
Make sure you are putting these ingredients together in the right relative dosages for the best results. Here’s a diagram with common interventions and their relative power to transform you from restricted to radiant:
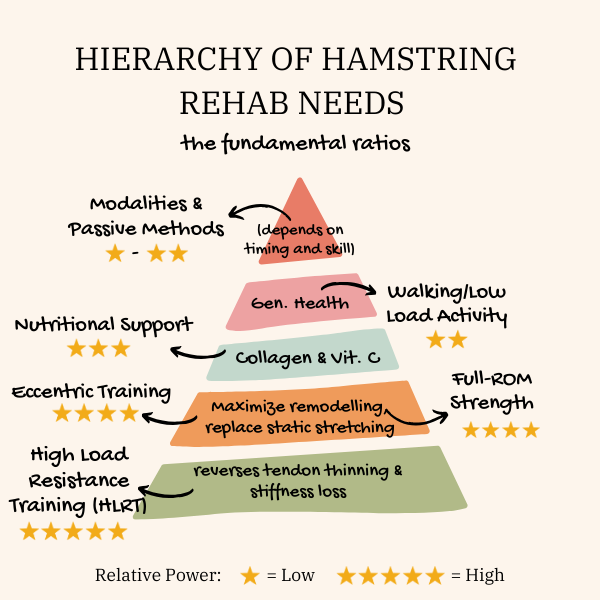
High-Load Resistance Training (HLRT)
Relative Power: ⭐⭐⭐⭐⭐
1–2 sessions/week
~80% of max capacity
5–8 reps
This is the most potent signal for reorganizing collagen and restoring tendon stiffness.
The catch: you must build toward it thoughtfully.
Examples: Hip thrusts, split lunges, dead lifts, bridges and nordics.
Eccentric-Focused Training
Relative Power: ⭐⭐⭐⭐☆
Slower lowering phases (3–5 seconds) exploit preserved eccentric strength and strongly stimulate tendon remodeling.
Examples: A ball bridge with a slow “roll-out” - letting your knees lengthen under tension for a knee-dominant move, and a slow forward single leg tip (aka a single leg RDL or “Tippy Bird”) with a dumbbell in your hand for a hip-dominant move.
Strength Training Over Stretching for Flexibility
Relative Power: ⭐⭐⭐⭐☆
Full-range strength training improves mobility and protects the new range.
Stretching alone improves sensation, not structure.
Example: The RDL is a great example of a move that can take your hamstring through a full range of motion. Do this instead of stretching and compare how you feel.
Nutritional Strategies: Collagen + Vitamin C (Adjunct)
Relative Power: ⭐⭐⭐☆☆
5-15g collagen
50mg vitamin C
~60 minutes before loading
Helpful, not essential. Some good evidence that supplementation improves collagen synthesis and health and shouldn’t be missed however exercise is still the main signal.
What about massage?
Massage and neuromotor techniques are valuable adjuncts, not foundations.
Used well, they can:
Reduce pain and threat
Improve movement confidence
Improve neuromuscular organization and self-use
Improve fluid dynamics and ease of motion
But early in healing, new collagen is fragile. Aggressive or poorly timed soft-tissue work can disrupt repair rather than support it. This is where injury timelines matter. Choose therapists who understand them.
I’ll admit something here: I love hands-on work. Whether I’m doing a cycling-style deep tissue session or guiding a neuromotor-focused Feldenkrais lesson, I find manual work deeply valuable and often transformative. It creates ease, clarity, and a sense of reconnection with the body that is hard to replicate any other way.
Still, this is where I see a common and costly error of proportion.
Hands-on work can make things feel better quickly. But if we lean on it too heavily, the tissue itself hasn’t changed enough to tolerate full load. That gap—between how good things feel and what the tissue can actually handle—is where re-injury happens and the downward spiral begins.
Do the soft-tissue and neuromotor work. Absolutely.
Just don’t let it replace the loading that actually restores resilience.
Should you stop activities that make you sore?
Not automatically.
High-speed, high-force movements should pause until baseline strength returns. That means high intensity running and sprinting, moves that require fast cutting or sudden changes of direction (this could be pickleball depending on your level - sorry!) or activities with inherent jumping (like many community exercise classes)
Low-to-moderate conditioning is extremely helpful if symptoms remain stable. Light to moderate intensity cycling is perfect, as is nordic skiing, walking and even easy jogging.
Avoid fear-based rest. Respect symptoms without surrendering capacity. From day one of an injury, you have two important jobs.
Healing the current injury is the obvious one. The second is easier to overlook: digging yourself out of the reduced-activity hole. The faster you recover, the less you need to modify your life. And the more strength, function, and control you maintain along the way, the less ground you have to reclaim later.
Closing: restoring trust in your body
High hamstring strains are unsettling because they sit at the crossroads of movement, power, and vulnerability. As tendon injuries, they often take appreciably longer to recover than muscle strains.
But they are also deeply trainable injuries.
With the right diagnosis, early loading, and progressive strength, these tissues don’t just heal — they adapt. You can make them stronger and more injury-proof than they were before.
This template works for most if not all soft tissue injuries. Do the right activities, include these ingredients and proportian them appropriately and have the confidence you are creating the right signals and the right environment to heal yourself.
The goal isn’t perfection.
It’s quiet competence.
It’s faith that these methods do work and they’ll work for you.
A hamstring you don’t think about.
A stride you trust again.
A body that feels capable, not fragile.
That’s the work.
Want help applying this to your own situation?
I offer one-on-one educational consultations for athletes navigating persistent or confusing injuries. These sessions are designed to help you make sense of what’s going on, understand your options, and build a smarter path forward alongside your local providers.
Consultations are informational and coaching-based, not physical therapy or medical treatment.
[Learn more or book a consult →]